Introduction
Background
Gastric cancer was once the second most common cancer in the world. In most developed countries, however, rates of stomach cancer have declined dramatically over the past half century. In the United States, stomach malignancy is currently the 14th most common cancer.
Decreases in gastric cancer have been attributed in part to widespread use of refrigeration, which has had several beneficial effects: increased consumption of fresh fruits and vegetables; decreased intake of salt, which had been used as a food preservative; and decreased contamination of food by carcinogenic compounds arising from the decay of unrefrigerated meat products. Salt and salted foods may damage the gastric mucosa, leading to inflammation and an associated increase in DNA synthesis and cell proliferation. Other factors likely contributing to the decline in stomach cancer rates include lower rates of chronic Helicobacter pylori infection, thanks to improved sanitation and use of antibiotics, and increased screening in some countries.1
Nevertheless, gastric cancer is still the second most common cause of cancer-related death in the world, and it remains difficult to cure in Western countries, primarily because most patients present with advanced disease. Even patients who present in the most favorable condition and who undergo curative surgical resection often die of recurrent disease. However, 2 studies have demonstrated improved survival with adjuvant therapy: a US study using postoperative chemoradiation2 and a European study using preoperative and postoperative chemotherapy.3
Anatomic aspects
The molecular biology responsible for carcinogenesis, tumor biology, and response to therapy in stomach cancer are active areas of investigation but are not addressed in this review. Instead, this article focuses on clinical management, which first requires a thorough understanding of gastric anatomy.
An image depicting stomach anatomy can be seen below.
Stomach and duodenum, coronal section.

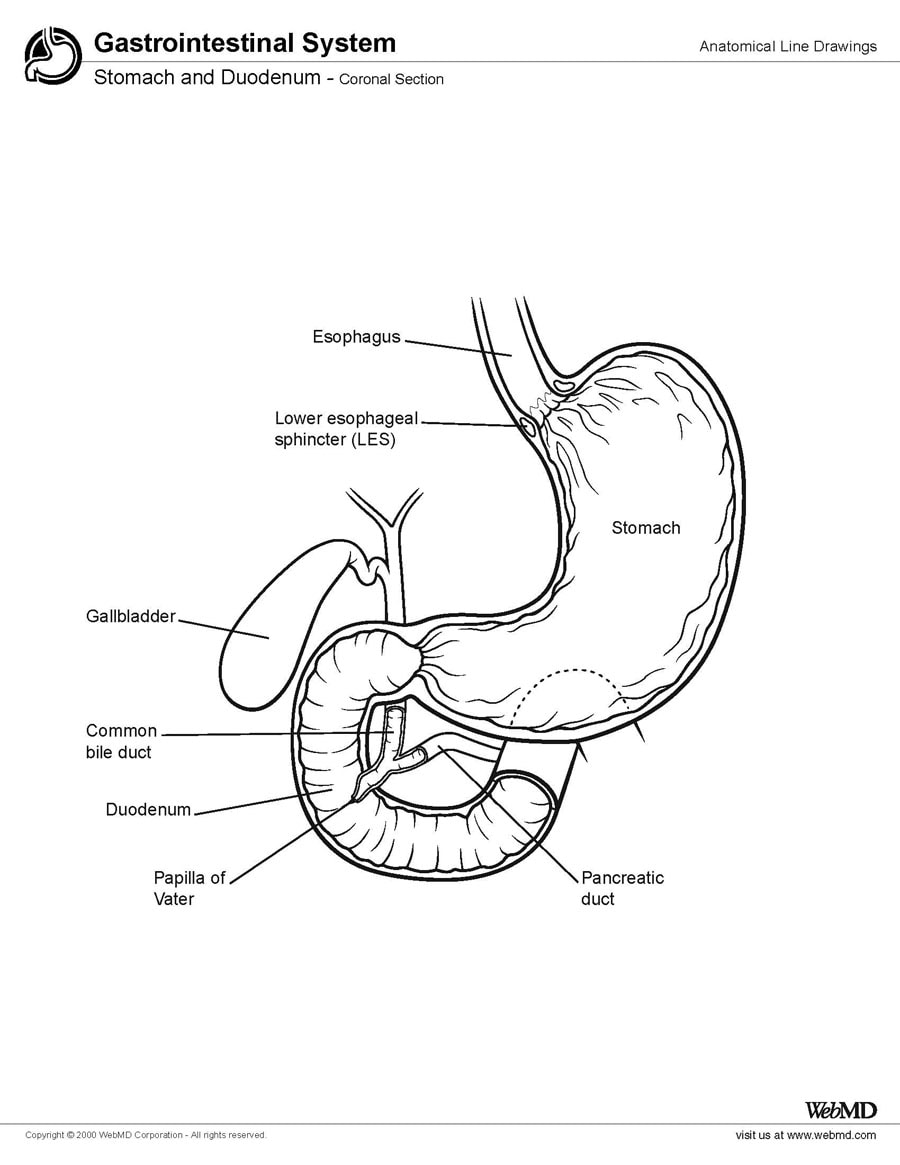
Stomach and duodenum, coronal section.
The stomach begins at the gastroesophageal junction and ends at the duodenum. The stomach has 3 parts: the uppermost part is the cardia; the middle and largest part is the body, or fundus; and the distal portion, the pylorus, connects to the duodenum. These anatomic zones have distinct histologic features. The cardia contains predominantly mucin-secreting cells. The fundus contains mucoid cells, chief cells, and parietal cells. The pylorus is composed of mucus-producing cells and endocrine cells.
The stomach wall is made up of 5 layers. From the lumen out, the layers include the mucosa, the submucosa, the muscularis layer, the subserosal layer, and the serosal layer. The peritoneum of the greater sac covers the anterior surface of the stomach. A portion of the lesser sac drapes posteriorly over the stomach. The gastroesophageal junction has limited or no serosal covering. The right portion of the anterior gastric surface is adjacent to the left lobe of the liver and the anterior abdominal wall. The left portion of the stomach is adjacent to the spleen, the left adrenal gland, the superior portion of the left kidney, the ventral portion of the pancreas, and the transverse colon.
The site of stomach cancer is classified on the basis of its relationship to the long axis of the stomach. Approximately 40% of cancers develop in the lower part, 40% in the middle part, and 15% in the upper part; 10% involve more than one part of the organ. Most of the decrease in gastric cancer incidence and mortality in the United States has involved cancer in the lower part of the stomach; the incidence of adenocarcinoma in the cardia has actually shown a gradual increase.
Pathophysiology
Ooi et al identified 3 oncogenic pathways that are deregulated in the majority (>70%) of gastric cancers: the proliferation/stem cell, NF-kappa β, and Wnt/beta-catenin pathways. Their study suggests that interactions between these pathways may play an important role in influencing disease behavior and patient survival.4
Understanding the vascular supply of the stomach allows understanding of the routes of hematogenous spread. The vascular supply of the stomach is derived from the celiac artery. The left gastric artery, a branch of the celiac artery, supplies the upper right portion of the stomach. The common hepatic artery branches into the right gastric artery, which supplies the lower portion of the stomach, and the right gastroepiploic branch, which supplies the lower portion of the greater curvature.
Understanding the lymphatic drainage can clarify the areas at risk for nodal involvement by cancer. The lymphatic drainage of the stomach is complex. Primary lymphatic drainage is along the celiac axis. Minor drainage occurs along the splenic hilum, suprapancreatic nodal groups, porta hepatis, and gastroduodenal areas.
Frequency
United States
The American Cancer Society estimates that 21,130 cases of gastric cancer will be diagnosed in 2009 (12,820 in men, 8,310 in women) and that 10,620 persons will die of the disease.5 Gastric cancer is the seventh leading cause of cancer deaths.
International
Once the second most common cancer worldwide, stomach cancer has dropped to fourth place, after cancers of the lung, breast, and colon and rectum. However, stomach cancer remains the second most common cause of death from cancer. The American Cancer Society estimates that in 2007 there were an estimated one million new cases, nearly 70% of them in developing countries, and about 800,000 deaths.1
Tremendous geographic variation exists in the incidence of this disease around the world. Rates of the disease are highest in Asia and parts of South America and lowest in North America.1 The highest death rates are recorded in Chile, Japan, South America, and the former Soviet Union.
Mortality/Morbidity
The 5-year survival rate for curative surgical resection ranges from 30-50% for patients with stage II disease and from 10-25% for patients with stage III disease. Because these patients have a high likelihood of local and systemic relapse, some physicians offer them adjuvant therapy. The operative mortality rate for patients undergoing curative surgical resection at major academic centers is less than 3%.
A review of 8 trials by Rothwell et al found allocation to aspirin reduced death caused by cancer. Individual patient data were available from 7 of the 8 trials. Benefit was apparent after 5 years of follow-up. The 20-year risk of cancer death was also lower in the aspirin group for all solid cancers. A latent period of 5 years was observed before risk of death was decreased for esophageal, pancreatic, brain, and lung cancers. A more delayed latent period was observed for stomach, colorectal, and prostate cancer. Benefit was only seen for adenocarcinomas in lung and esophageal cancers. The overall effect on 20-year risk of cancer death was greatest for adenocarcinomas.6
Race
The rates of gastric cancer are higher in Asian and South American countries than in the United States. Japan, Chile, and Venezuela have developed a very rigorous early screening program that detects patients with early stage disease (ie, low tumor burden). These patients appear to do quite well. In fact, in many Asian studies, patients with resected stage II and III disease tend to have better outcomes than similarly staged patients treated in Western countries. Some researchers suggest that this reflects a fundamental biologic difference in the disease as it manifests in Western countries.
In the United States, Asian and Pacific Islander males and females have the highest incidence of stomach cancer, followed by black, Hispanic, white, American Indian, and Inuit populations.
Sex
In the United States, gastric cancer affects slightly more men than women; the American Cancer Society estimates that in 2009, 12,820 new cases will occur in men and 8,310 in women.5 Worldwide, however, gastric cancer rates are about twice as high in men as in women.1
Age
Most patients are elderly at diagnosis. The median age for gastric cancer in the United States is 70 years for males and 74 years for females. The gastric cancers that occur in younger patients may represent a more aggressive variant or may suggest a genetic predisposition to development of the disease.
Clinical
History
In the United States, about 25% of stomach cancer patients present with localized disease, 31% present with regional disease, and 32% present with distant metastatic disease; the remainder of cases surveyed were listed as unstaged.
Early disease has no associated symptoms; however, some patients with incidental complaints are diagnosed with early gastric cancer. Most symptoms of gastric cancer reflect advanced disease. Patients may complain of indigestion, nausea or vomiting, dysphagia, postprandial fullness, loss of appetite, melena, hematemesis, and weight loss.
Late complications include pathologic peritoneal and pleural effusions; obstruction of the gastric outlet, gastroesophageal junction, or small bowel; bleeding in the stomach from esophageal varices or at the anastomosis after surgery; intrahepatic jaundice caused by hepatomegaly; extrahepatic jaundice; and inanition resulting from starvation or cachexia of tumor origin.
Physical
All physical signs are late events. By the time they develop, the disease is almost invariably too far advanced for curative procedures.
Signs may include a palpable enlarged stomach with succussion splash; hepatomegaly; periumbilical metastasis (Sister Mary Joseph nodule); and enlarged lymph nodes such as Virchow nodes (ie, left supraclavicular) and Irish node (anterior axillary). Blumer shelf (ie, shelflike tumor of the anterior rectal wall) may also be present. Some patients experience weight loss, and others may present with melena or pallor from anemia.
Paraneoplastic syndromes such as dermatomyositis, acanthosis nigricans, and circinate erythemas are poor prognostic features.
Other associated abnormalities also include peripheral thrombophlebitis and microangiopathic hemolytic anemia.
Causes
Gastric cancer may often be multifactorial, involving both inherited predisposition and environmental factors.7 Environmental factors implicated in the development of gastric cancer include diet, Helicobacter pylori infection, previous gastric surgery, pernicious anemia, adenomatous polyps, chronic atrophic gastritis, and radiation exposure.
Diet
A diet rich in pickled vegetables, salted fish, salt, and smoked meats correlates with an increased incidence of gastric cancer.7
A diet that includes fruits and vegetables rich in vitamin C may have a protective effect.8
Smoking
Smoking is associated with an increased incidence of stomach cancer in a dose-dependent manner, both for number of cigarettes and for duration of smoking.
Smoking increases the risk of cardiac and noncardiac forms of stomach cancer.9 Cessation of smoking reduces the risk.
A meta-analysis of 40 studies estimated that the risk was increased by approximately 1.5- to 1.6-fold and was higher in men.10
Helicobacter pylori infection
Chronic bacterial infection with H pylori is the strongest risk factor for stomach cancer.
H pylori may infect 50% of the world's population, but many fewer than 5% of infected individuals develop cancer. It may be that only a particular strain of H pylori is strongly associated with malignancy, probably because it is capable of producing the greatest amount of inflammation. In addition, full malignant transformation of affected parts of the stomach may require that the human host have a particular genotype of interleukin (IL) to cause the increased inflammation and an increased suppression of gastric acid secretion. For example, IL-17A and IL-17F are inflammatory cytokines that play a critical role in inflammation. Wu et al found that carriage of IL-17F 7488GA and GG genotypes were associated with an increased risk of gastric cancer.11
H pylori infection is associated with chronic atrophic gastritis, and patients with a history of prolonged gastritis have a sixfold increased risk of developing gastric cancer. Interestingly, this association is particularly strong for tumors located in the antrum, body, and fundus of the stomach but does not seem to hold for tumors originating in the cardia.12
Previous gastric surgery
Previous surgery is implicated as a risk factor. The rationale is that surgery alters the normal pH of the stomach, which may in turn lead to metaplastic and dysplastic changes in luminal cells.13
Retrospective studies demonstrate that a small percentage of patients who undergo gastric polyp removal have evidence of invasive carcinoma within the polyp. This discovery has led some researchers to conclude that polyps might represent premalignant conditions.
Genetic factors
Some 10% of stomach cancer cases are familial in origin.
Genetic factors involved in gastric cancer remain poorly understood, though specific mutations have been identified in a subset of gastric cancer patients. For example, germline truncating mutations of the E-cadherin gene (CDH1) are detected in 50% of diffuse-type gastric cancers, and families that harbor these mutations have an autosomal dominant pattern of inheritance with a very high penetrance.14
Other hereditary syndromes with a predisposition for stomach cancer include hereditary nonpolyposis colorectal cancer, Li-Fraumeni syndrome, familial adenomatous polyposis, and Peutz-Jeghers syndrome.
Epstein-Barr virus
The Epstein-Barr virus may be associated with an unusual (<1%)>
Pernicious anemia
Pernicious anemia associated with advanced atrophic gastritis and intrinsic factor deficiency is a risk factor for gastric carcinoma.
Gastric ulcers
Gastric cancer may develop in the remaining portion of the stomach following a partial gastrectomy for gastric ulcer.
Benign gastric ulcers may themselves develop into malignancy.
Obesity
Obesity increases the risk of gastric cardia cancer.
Radiation exposure
Survivors of atomic bomb blasts have had an increased rate of stomach cancer. Other populations exposed to radiation may also have an increased rate of stomach cancer.
A large cohort study examined whether use of oral bisphosphonates was associated with an increased risk of esophageal or gastric cancers. No significant difference was observed for increased risk of esophageal or gastric cancers between the bisphosphonate cohort and the control group


0 commentaires:
Post a Comment